Author: Doctor Paolo Pirozzi
Clinical Model
Shoulder Tendon Traumatic Injury: rock climbing has become a professional competitive sport in recent years and recent months also an Olympic discipline. This has generated attention around the discipline that has also involved many non-professional people, leading them to practice climbing at an amateur level both on natural and artificial walls, often without sufficient athletic training, creating deficits in flexibility, strength. , resistance, agility, and balance: this, due to the important stress to which the joints of the upper limb are subjected (shoulders, elbows, hand phalanges), has led to an exponential increase in injuries derived from climbing, both of, such as muscle-tendon injuries and detachments of the tendon pulleys of the hand flexors, both of over-use origin, such as insertional tendinopathies of the elbow. Furthermore, climbing requires a high level of mental control which generates an additional point of challenge for the athlete himself, with a consequent increase in the psycho-physical stress to which the climber’s body is subjected. [1,2]

Patient Profile
The target of the professional sportsman varies by age and climbing experience: for example, in a study by Klauser et al, on 34 climbers examined their age ranged from 21 to 54 years (mean ± SD, 29.7 ± 8.3) , their climbing experience ranged from 5 to 25 years, and their climbing level ranged from 7 to 11 on the UIAA (Union Internationale des Associations d’Alpinisme, levels 1 to 11) scale [3]. As for the patient’s medical history of the clinical case taken into consideration, he is a 58-year-old man, an amateur sports climbing athlete with less than 10 years of experience, who suffered an injury one month before the evaluation during an outdoor route: in fact As he tries to grab a hook on his right to continue climbing, he feels a stabbing, stabbing pain on the inside of his shoulder. Despite the traumatic nature of the injury and pain, the patient underestimates the injury and does not carry out a specialist visit or a diagnostic assessment. He comes to the office one month after the injury to his right shoulder, with pain during maximum abduction but especially during maximum shoulder flexion.
Pain localization
The pain occurred in the insertion area of the supraspinatus tendon, just distal from its passage under the acromial bridge: the insertion of the supraspinatus is usually easily palpable and inspectable by the operator and guarantees important diagnostic information.
Symptomatic Characteristics
The pain manifests itself in a dull and non-continuous way, with greater intensity in the morning upon waking up and in the evening after a day of work and training; besides, the intensity of pain increases significantly during shoulder movements of maximum abduction and especially maximum flexion and even more so if the position of maximum abduction or flexion is maintained for a few seconds. This situation affected the patient’s mental well-being, as it led him to limit his daily activities a lot for fear of pain and its worsening.
Physical-Clinical Exam (if possible, accompany with photos with informed consent):
- Inspection: no visible signs of muscle-tendon injury
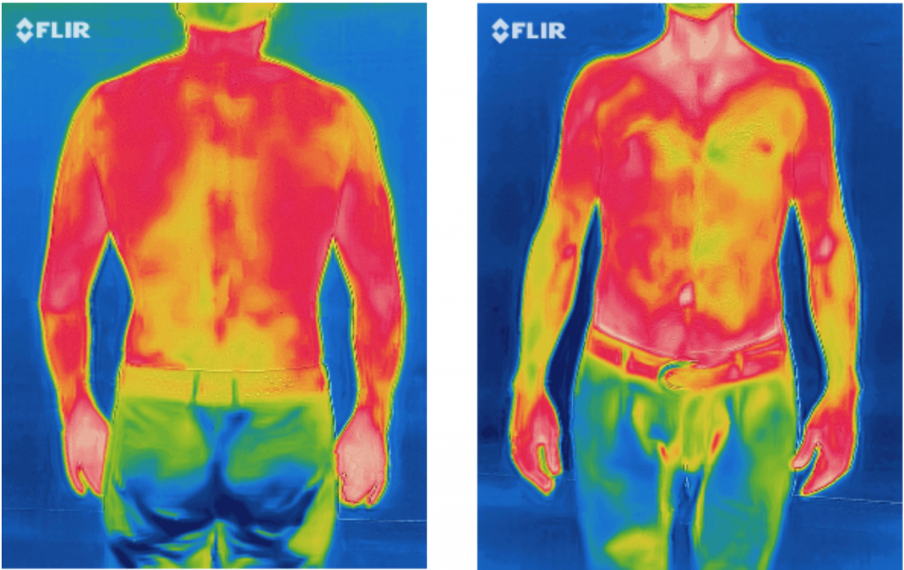
- Thermography: visible alteration of the distribution of body heat (see photo)
- Palpation: Pain on palpation of the supraspinatus tendon in the mid-insertional portion
- Active tests: ROM active and with Baiobit with increased pain in the last degrees of shoulder abduction and flexion
- Passive examinations: no pain during PROM, slight limitation in the last degrees of joint mobility on all planes
- Functional and specific tests: JOBE’s test for positive supraspinatus with increased painful symptoms
- Neurological tests: not provided

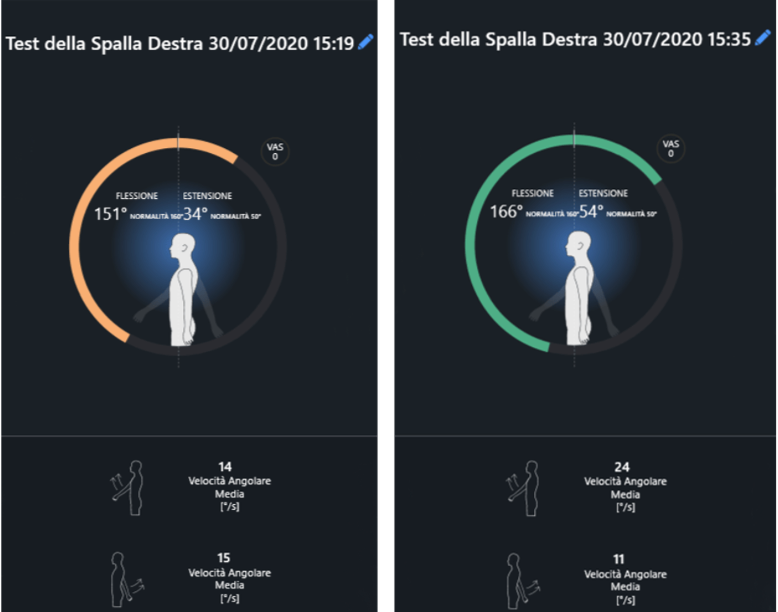
Test with Baiobit:
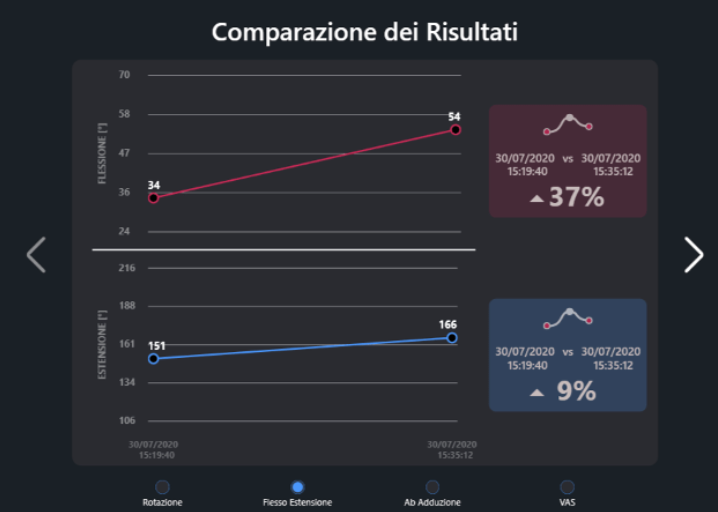
As anticipated before, we assessed the shoulder range of motion through the Baiobit sensor immediately before and immediately after an analgesic stimulus on the insertion of the supraspinatus: the increase in joint widths (by 37% in flexion and 9% in extension) and angular velocity in flexion, at a distance of only 15 minutes between the two evaluations, confirm the precise point where the patient suffered the injury. Furthermore, when examining the abduction force with a manual dynamometer, comparing with the non-injured left shoulder which generated a force of 137 Newton, the injured right shoulder generated a force of 97 Newton before the analgesic stimulus and a force of 117.5 Newton after analgesic stimulation, with an increase in strength of 18%.
Recommended Instrumental Exams
With the data acquired during the initial evaluation, the therapeutic indication was to proceed with a diagnostic investigation of the lesion through magnetic resonance imaging before starting a rehabilitation process, to be more effective and decisive. The magnetic resonance has confirmed the lesion of the tendon of the superaspinosus; this is the excerpt: “[…] Signal inhomogeneity of the supraspinatus tendon in the insertional and pre-insertional site as for mild tendinosis. In the posterior insertion site, a thin hyperintense linear image of about 5 mm, compatible with partial tendon injury, is appreciated. The trophism of the relative muscular belly has been preserved. […] “.
Etiology
Acute injury due to uncontrolled movement of grip on rock with the right hand.
Treatment
A meta analysis by Anssi et al points out that there is no clinically significant difference between surgery and active physiotherapy in the 1-year follow-up to improve the Constant-Murley score (introduced to determine function after treatment of a shoulder injury) or reduce pain caused by the rotator cuff tear. Since physiotherapy is less prone to complications and less expensive than surgery, a conservative approach is recommended as the initial treatment modality for rotator cuff tears [4]. Even in the specific lesion of the supraspinatus conservative treatment can be a primary treatment method consisting in the recovery of joint mobility, proprioceptive recovery, muscle strengthening and stretching in the post-healing phase of the wound [5].
In the specific case treated here, the rehabilitation program was characterized by a functional re-education path of the shoulder, with particular attention to improving thoracic mobility in extension and rotation to gain the missing degrees in shoulder movement and to increasing the tendon tightness of the shoulder. supraspinatus muscle during the typical movements of the climbing gesture, i.e. all overhead movements, especially in traction rather than thrust. For this reason, the movements mainly explored were:
- Horizontal shoulder pull with elbow flexed first and elbow extended then, with progressive increase in resistance during exercise
- Vertical shoulder traction with elbow flexed first and elbow extended then, with progressive increase in resistance during exercise
- Vertical shoulder thrust with elbow flexed first and elbow extended then, with progressive increase in resistance during exercise
- Shoulder stabilization in body load, both in bilateral and unilateral support
- Exercises with Baiobit
- Shoulder Range of Motion assessment, comparing injured shoulder before and after analgesic stimulus, pre and post rehabilitation.
Results
At the end of the rehabilitation process, which lasted 7 weeks with 2 sessions per week for a total of about 15 sessions, the patient fully gained joint mobility, improved motor control of the shoulder and arm and consequently increased his athletic and fitness abilities. performance: as an amateur climbing athlete, he managed to perform increasingly difficult training courses without feeling any type of fatigue or shoulder pain. In this clinical case, the Baiobit sensor proved to be a reliable tool for increasing the information necessary for a precise and correct functional evaluation of a damaged tendon: moreover, by precisely quantifying important data such as degrees of movement and angular velocities, it significantly increases adherence. to the patient’s rehabilitation process, thus maximizing short and long-distance outcomes.
References:
- Schöffl, Volker & Schöffl, Isabelle & Frank, L. & Küpper, Thomas & Simon, M. & Lutter, Christoph. (2020). Tendon Injuries in the Hands in Rock Climbers:Epidemiology, Anatomy, Biomechanics and Treatment An Update. Muscle Ligaments and Tendons Journal. 10. 233. 10.32098/mltj.02.2020.08.
- Cole, Keegan P. MD; Uhl, Richard L. MD; Rosenbaum, Andrew J. MD Comprehensive Review of Rock Climbing Injuries, Journal of the American Academy of Orthopaedic Surgeons: June 15, 2020 – Volume 28 – Issue 12 – p e501-e509 doi: 10.5435/JAAOS-D-19-00575.
- Klauser, Andrea & Bodner, Gerd & Frauscher, Ferdinand & Gabl, M & Nedden, D. (1999). Finger injuries in extreme rock climbers. Assessment of high-resolution ultrasonography. The American journal of sports medicine. 27. 733-7. 10.1177/03635465990270060801.
- Ryösä, Anssi & Laimi, Katri & Äärimaa, Ville & Lehtimäki, Kaisa & Kukkonen, Juha & Saltychev, Mikhail. (2016). Surgery or conservative treatment for rotator cuff tear: a meta-analysis. Disability and Rehabilitation. 39. 1-7. 10.1080/09638288.2016.1198431.
- 5. Edwards P, Ebert J, Joss B, Bhabra G, Ackland T, Wang A. EXERCISE REHABILITATION IN THE NON-OPERATIVE MANAGEMENT OF ROTATOR CUFF TEARS: A REVIEW OF THE LITERATURE. Int J Sports Phys Ther. 2016;11(2):279-301