Author: Dr. Alessio Liberati
Low back pain is generally defined as "a painful symptomatology perceived in the posterior region of the spine, in the stretch between the lower edge of the costal arch and the lower gluteal folds" [1]. It represents the most common musculoskeletal disease in the world [2], followed in second place by neck pain. Estimates from the Global Burden of Diseases tell us that its lifetime prevalence is between 49% and 90% [3] and that the recurrence rate, one year after the first episode, is just over 30% [4]. Furthermore, to fully understand the extent of this pathology, it is good to remember that lumbar problems are an important cause of disability. This is enough to say that only in America the total costs related to this pathology are estimated at around 100 billion dollars [5].
Low back pain is an extremely varied and complex pathology. Therefore, a thorough evaluation of the Range Of Motion (ROM) is necessary, both at the lumbar level and in the adjacent body districts. In these cases, the use of reliable instruments is strongly recommended, as it would be difficult to quantify spinal and joint movements with visual inspection alone [6]. For a return to normal daily life, the guidelines recommend minimizing inactivity and indicate therapeutic exercise among the most effective therapies [7]. The latter is useful from the early stages of the assessment, as it allows pain management by acting on its modulatory mechanisms [8].
Anamnesis
61-year-old man, active standard of living, diagnosed with Lumbosciatalgia. The pain occurs mainly during the sitting position, the supine position and in the execution of trunk movements on all planes of space, especially to the front.
Assessment
During the first session, the following tests are performed:
Test ROM of the trunk with baiobit
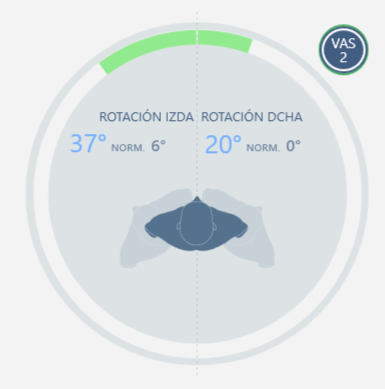
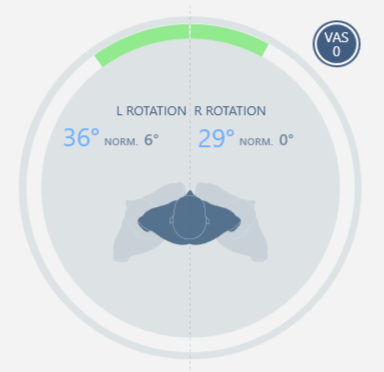
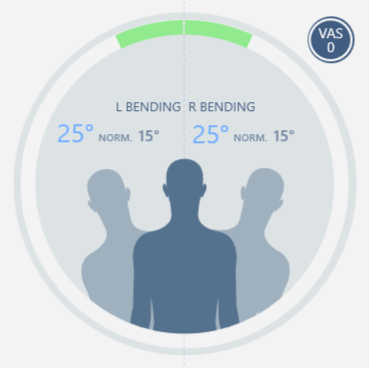
Objective ROM measurement performed on the three planes of movement, from which it is highlighted (Figure 1):
- left rotation 37°, right rotation 20° with VAS pain 2/10
- 44° flexion, 20° extension without pain
- left bend 15°, right bend 7° with 6/10 VAS pain
The examination reveals a limitation of movement in the lateral flexion associated with pain.
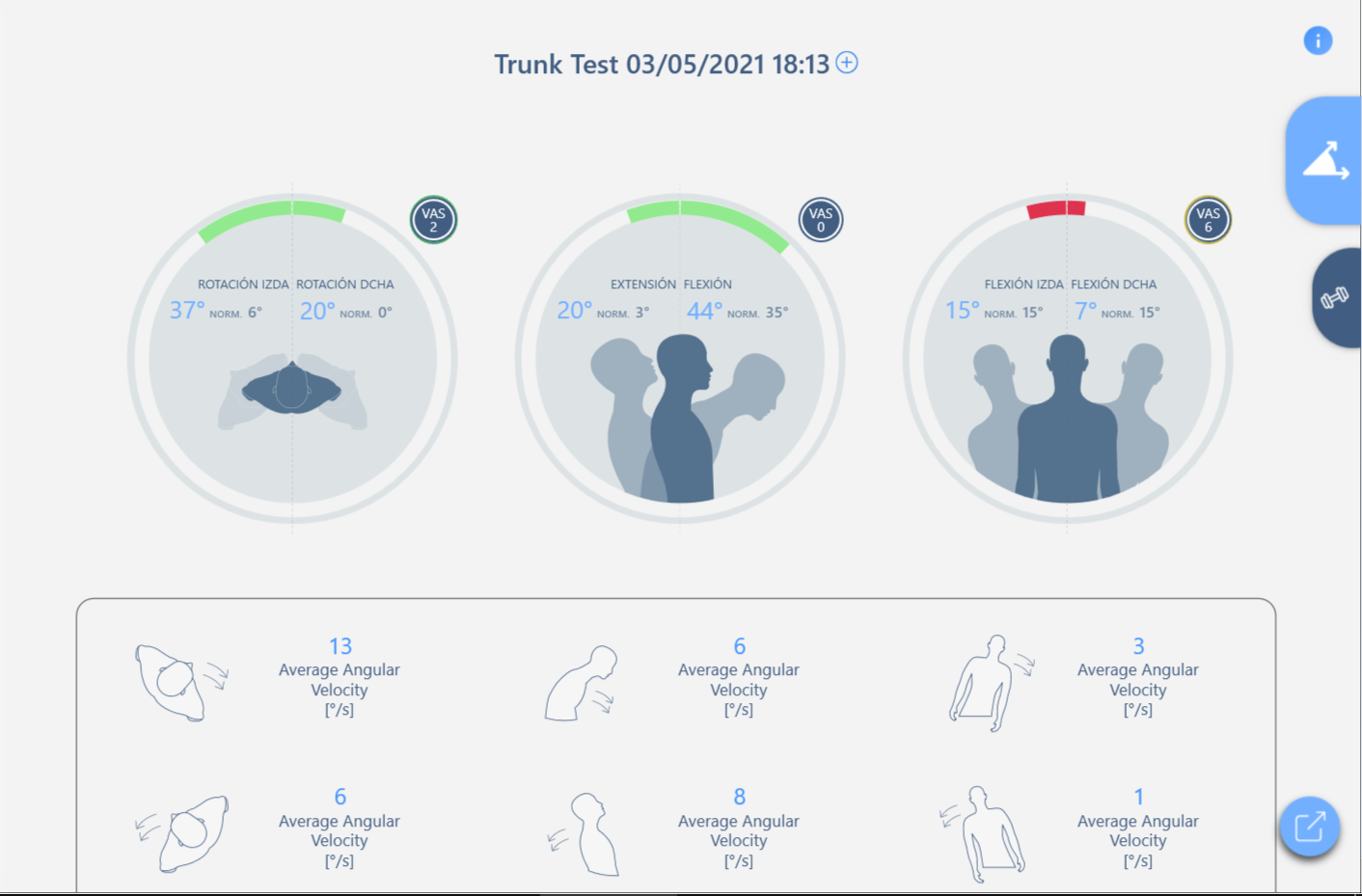
Figure 1 - First Assessment
Lasegue test with baiobit
This test was performed with the FREE baiobit test to objectively measure the maximum degrees of hip flexion. A positive test emerges with the appearance of pain at 34°.
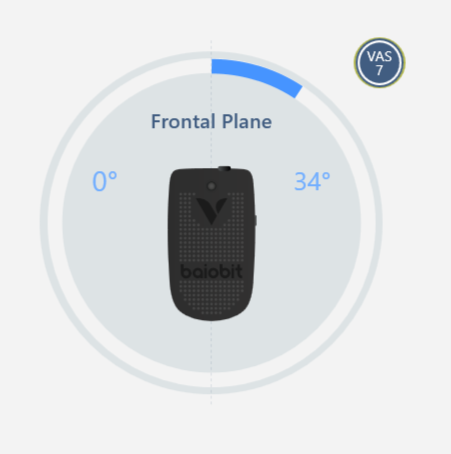
Figure 2 - First Test Lasegue
Myofascial tests
Used to identify altered fascial components that can generate stiffness and tension. At the end of the physiotherapy evaluation and after medical consultation, an altered descending fascial component is hypothesized, which generates stiffness in the lumbar region associated with compression of the sciatic nerve.
Rehabilitation program
We therefore propose a rehabilitation program consisting of a session with fascial manipulation treatment, followed by two weeks of independent exercises at home with a frequency of 3 times a week.
Exercises assigned at home through the use of the baiobit software (Figure 3):
· bird dog
· plank
· side deck
· hip abduction while standing
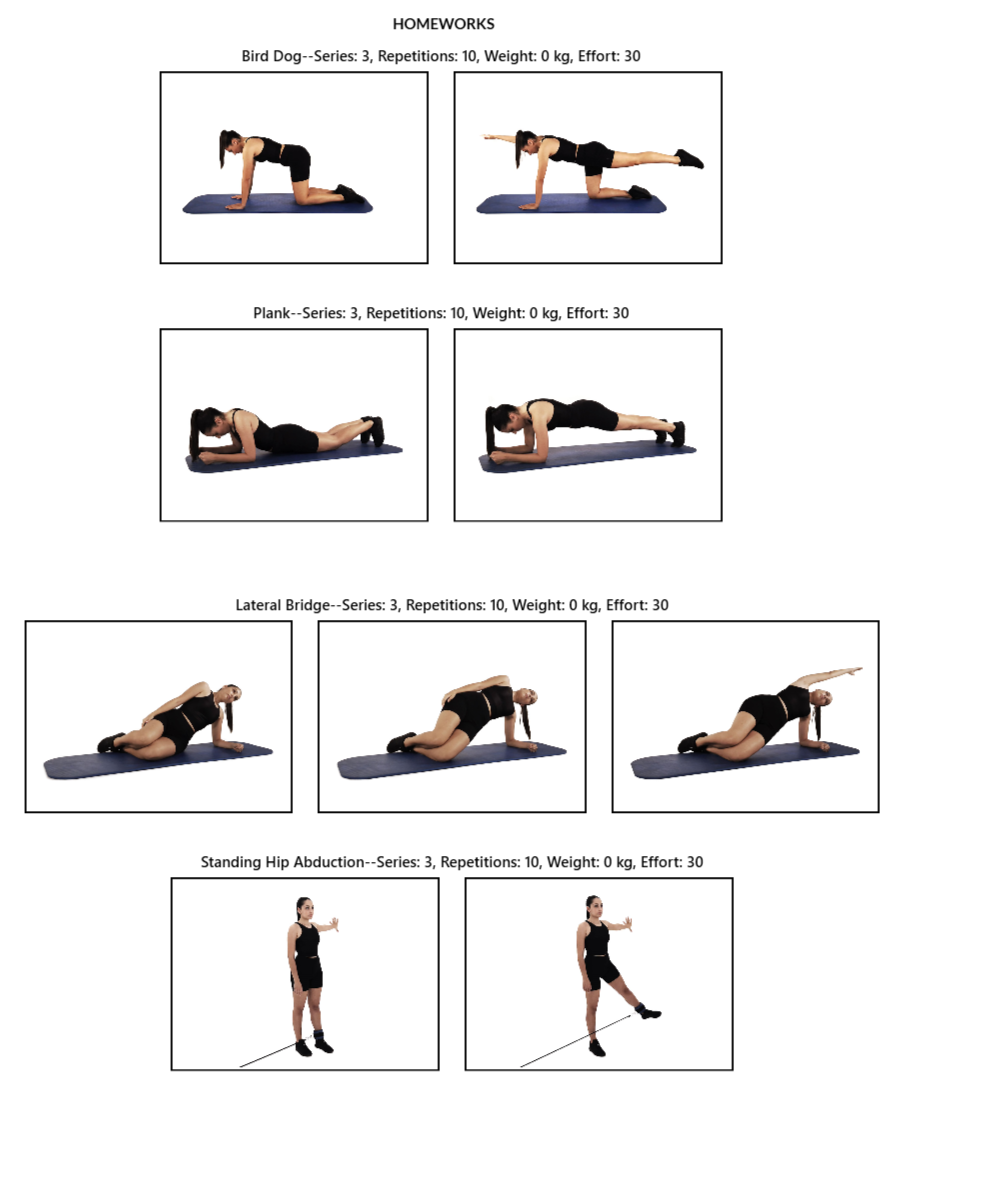
Figure 3 - Home exercises
Results
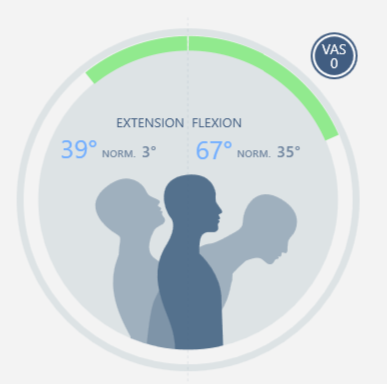
At the end of the therapy, a re-evaluation is carried out, in particular the ROM test of the trunk is carried out again, which shows a clear improvement in the range of motion on the most compromised planes.
| Initial evaluation | Final evaluation |
Left and right rotation |
| 
|
Flexion-Exstention | 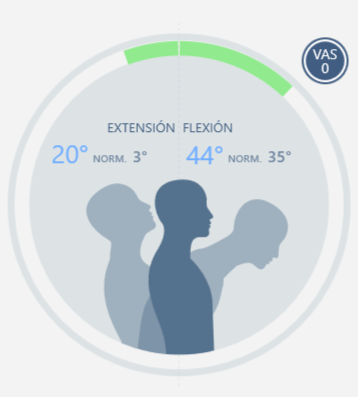
|
|
Latero flexion left and right
|

|  |
In addition, the Lasegue test is re-evaluated, which shows a clear decrease in VAS 2 tenderness and an improvement in the range of motion up to 60 ° (Figure 5).
Figure 5 - Test di Lasegue outcome
Bibliography
[1] Burton AK. European guidelines for prevention in low back pain. COST B13 Working Group. 2004: 1-53.
[2] Blyth, F. M., Briggs, A. M., Schneider, C. H., Hoy, D. G., & March, L. M. (2019). The Global Burden of Musculoskeletal Pain—Where to From Here? American Journal of Public Health, 109(1), 35–40.
[3] Scott, N.A., C. Moga, and C. Harstall. Managing low back pain in the primary care setting: the know-do gap. Pain Res Manag, 2010. 15(6): p. 392-400.
[4] Da Silva, T., et al., Risk of Recurrence of Low Back Pain: A Systematic Review. J Orthop Sports Phys Ther, 2017. 47(5): p. 305-313.
[5] Dieleman JL, Baral R, Birger M et al (2016) Us spending on personal health care and public health, 1996–2013. JAMA 316(24):2627–26469.
[6] K. G. B. S. G. R. Mayer TG, « Spinal range of motion. Accuracy and sources of error with inclinometric measurement,» Spine, vol. 22, pp. 1976-84, 1997.
[7] B. J. C. C. e. a. Airaksinen O, «European guidelines for the management of chronic nonspecific low back pain,» Eur Spine J, Vol. %1 di %25:192-300, 2006.
[8] H. B. V. a. M. D. Jones, «Exercise-induced hypoalgesia after acute and regular exercise: experimental and clinical manifestations and possible mechanisms in individuals with and without pain,» Pain Rep,, vol. 5, 2020.